

Congenital heart defect (CHD) terjadi pada sekitar 1% kelahiran hidup, atau 8 dari setiap 1000 kelahiran. Terdapat 25.000 bayi yang lahir setiap tahunnya dengan penyakit CHD, dan lebih dari 1.000.000 bayi telah mencapai usia dewasa dan tinggal di Amerika Serikat dengan penyakit CHD yang signifikan secara fungsional.
Kelainan jantung bawaan dapat dideteksi ketika ukuran jantung tidak lebih besar dari kacang tanah dan sudah berkembang sempurna. Pada sebagian besar bayi dengan CHD, terdapat spekulasi bahwa faktor genetik berperan dalam terjadinya cacat tersebut, namun pola pewarisannya masih belum jelas.
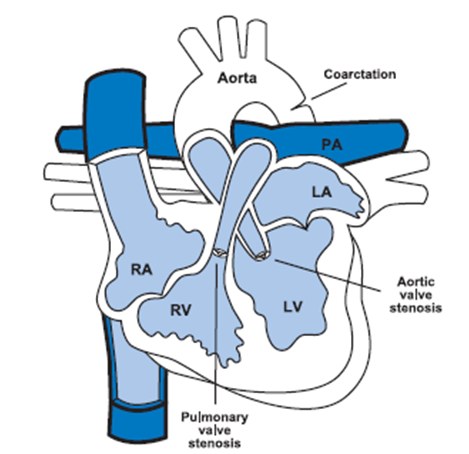
Secara umum, congenital heart defect dibagi kedalam dua kelompok uatama, yaitu Acyanotics Congenital Heart Defect dan Cyanotic Congenital Heart Defect. Cyanotic menyebabkan saturasi oksigen dalam darah menurun, sedangkan Acyanotic tidak mengubah saturasi oksigen dalam darah. Lesi acyanotic dapat menyebabkan masalah penyumbatan aliran darah ke bilik jantung (masalah tekanan) atau permasalahan pada volume darah yang mengalir melalui bilik jantung kembali ke paru-paru (masalah volume).
Acyanotics Congenital Heart Defect
Acyanotics Congenital Heart Defect (A-CHD) menyebabkan peningkatan volume darah yang mengalir ke paru-paru. Hal ini mengindikasikan adanya kontak antara sisi sirkulasi darah sistemik dan paru di jantung dan mengakibatkan aliran darah yang teroksigenasi penuh masuk kembali ke paru-paru. Kelainan jantung yang termasuk A-CHD adalah atrial septal defects (ASDs), ventricular septal defects (VSDs), atrioventricular septal defects (AVSDs), and patent ductus arteriosus (PDA).
1. Atrial Septal Defects (ASD)
Pada kondisi ASD, terdapat lubang pada dinding yang memisahkan atrium. Hal ini disebabkan oleh paten foramen ovale, yaitu lubang berbentuk oval di dinding atrium yang seharusnya menutup segera setelah lahir. Foramen tersebut memang ada secara alami pada septum atrium di dalam rahim yang menghubungkan atrium kanan dan kiri dan akan menutup segera setelah lahir. Namun dapat terjadi kondisi yang disebut ostium sekundum, jika foramen ovale lebih besar dari yang seharusnya, atau jika lipatan jaringan yang seharusnya menutup foramen tersebut tergeser atau kurang. Hal ini menyebabkan foramen tidak tertutup dan terdapat kebocoran pada dinding pemisah atrium. Tanpa penutupan dan berlangsung selama bertahun-tahun, tekanan rendah pada tingkat atrium akan mengakibatkan pembesaran atrium dan ventrikel kanan secara bertahap.Gejala dari ASD biasanya murmur jantung, ventrikel kanan yang terlalu aktif, dan arteri pulmonalis yang membesar.
2. Ventricular Sepal Defects (VSD)
Dinding ventrikel terdiri dari tiga area berbeda yang menyatu membentuk dinding otot padat tunggal ventrikel. VSD terjadi saat terdapat lubang pada dinging ventrikel. Dengan VSD, sebagian darah kaya oksigen di ventrikel kiri yang seharusnya dipompa ke seluruh tubuh melalui aorta dikeluarkan langsung ke ventrikel kanan melalui lubang di dinding ventrikel tersebut. Pada kondisi luban yang besar, banyak darah yang akan masuk ke paru-paru dan menyebabkan paru-paru tersumbat dan sesak napas. Sejumlah besar darah akan kembali dari paru-paru ke jantung kiri, yang kemudian menjadi terbebani jantung kiri dan akhirnya membesar. Pada kondisi VSD yang besar, mungkin muncul gejala seperti dispnea, kesulitan makan, pertumbuhan yang buruk, keringat berlebih, infeksi paru berulang, gagal jantung pada masa bayi awal, gangguan pernapasan, dan kegagalan pertumbuhan
3. Atrioventricular Septal Defect (AVSD)
AVSD merupakan kelainan jantung di mana terdapat lubang antara bilik jantung kanan dan kiri, dan katup yang mengontrol aliran darah antar bilik tersebut mungkin tidak terbentuk dengan benar. AVSD lengkap melibatkan bagian jantung di mana dinding atrium bertemu dengan dinding ventrikel dan katup jantung (mitral/trikuspid). Hal ini menyebabkan terbentuknya lubang besar yang membentang di dinding jantung dengan satu katup besar di kedua sisinya. Gejalanya meliputi kongesti paru-paru dan hipertensi pulmonal. Akibatnya anak menjadi kurus akibat kerja pernafasan yang meningkat. Hal ini terkait dengan down syndrome, dan sekitar 25% orang dengan down syndrome memiliki AVSD.
4. Patent Ductus Arteriosus (PDA)
PDA merupakan kelainan jantung yang terjadi saat terdapat saluran penghubung antara aorta dan arteri pulmonalis. Duktus arteriosus (DA) merupakan jalur normal sirkulasi darah janin yang menghubungkan arteri pulmonalis dan aorta desendens. Saluran ini sejatinya memang ada sejak lahir, namun akan menutup seiring pertumbahan bayi. Ketika jumlah oksigen dalam darah meningkat setelah kelahiran, tubuh berhenti memproduksi prostaglandin E1, yang membuat DA tetap terbuka, dan DA akan menutup beberapa jam setelah kelahiran dan menutup secara permanen dalam beberapa minggu pertama.Pada kondisi PDA, saluran ini tidak menutup dan akhirnya menyebabkan terjadinya aliran darah pada aorta dan arteri pulmonalis. PDA dikaitkan dengan rubella ibu dan prematuritas.Perbedaan tekanan antara sisi kiri dan kanan jantung menyebabkan terlalu banyak darah yang masuk ke paru-paru. Gejala yang ditimbulkan bergantung pada ukuran pembukaan dan derajat prematuritas. Pembukaan yang besar dapat menyebabkan kongesti paru, CHF, dan edema.
Cyanotic Congenital Heart Defect
Cyanotic Congenital Heart Defect (C-CHD) menyebabkan penurunan saturasi oksogen dalam darah. Gejala khas pada kondisi ini adalah adanya sianois, suatu kondisi kekurangan oksigen yang menyebabkan bibir, kuku, dan ujung jari menjadi kebiruan. Karena desaturasi oksigen arteri yang kronis, tubuh merangsang eritropoiesis atau peningkatan pembentukan sel darah merah, yang mengakibatkan polisitemia. Polisitemia adalah suatu kondisi kelebihan sel darah merah, yang meningkatkan kekentalan darah dan meningkatkan risiko gangguan serebrovaskular dan masalah mikrovaskuler pada individu tersebut. Cyanotic Congenital Heart Defect termasuk tetralogy of Fallot (TOF), double-outlet right ventricle, and hypoplastic left heart syndrome
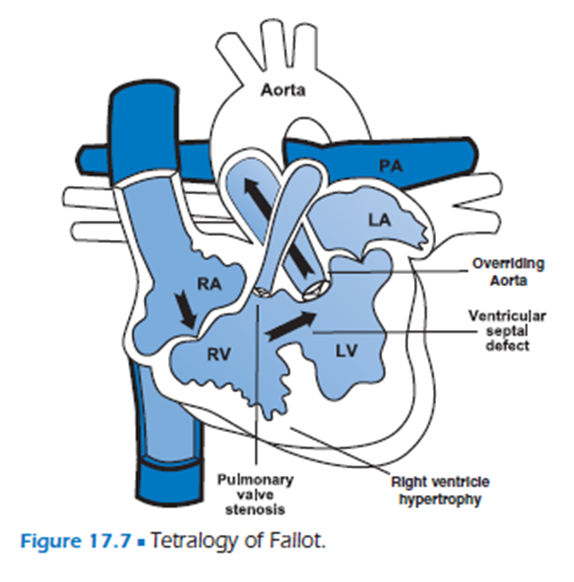
1. Tetralogy of Fallot (TOF)
TOF memiliki empat komponen dasar dan merupakan kelainan jantung bawaan sianotik yang paling umum terjadi.1 Komponen dasar pertama adalah VSD berukuran besar dengan darah bercampur bebas di antara kedua ventrikel. Komponen kedua adalah stenosis pulmonal, yang menyebabkan penyumbatan pada paru-paru atau penyumbatan saluran keluar ventrikel kanan. Komponen ketiga adalah aorta yang terletak di atas VSD (disebut overriding aorta). Terakhir, terjadi hipertrofi ventrikel kanan yang disebabkan oleh peningkatan tekanan akibat obstruksi aliran keluar ventrikel kanan. Aliran darah ke arteri pulmonalis terhambat, sehingga darah yang miskin oksigen lebih mudah masuk ke aorta dibandingkan ke arteri pulmonalis. Akibatnya adalah rendahnya kadar oksigen di arteri dan jaringan tubuh. Hal ini mengakibatkan sianosis dengan gejala mudah lelah, pingsan, dan syok.
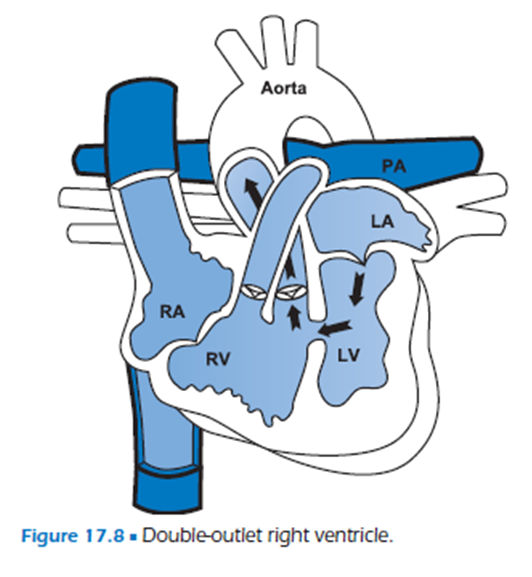
2. Double-outlet Right Ventricle
Pada Double-outlet Right Ventricle, aorta dan arteri pulmonalis muncul dari ventrikel kanan. Satu-satunya jalan keluar dari ventrikel kiri adalah melalui VSD ke ventrikel kanan.
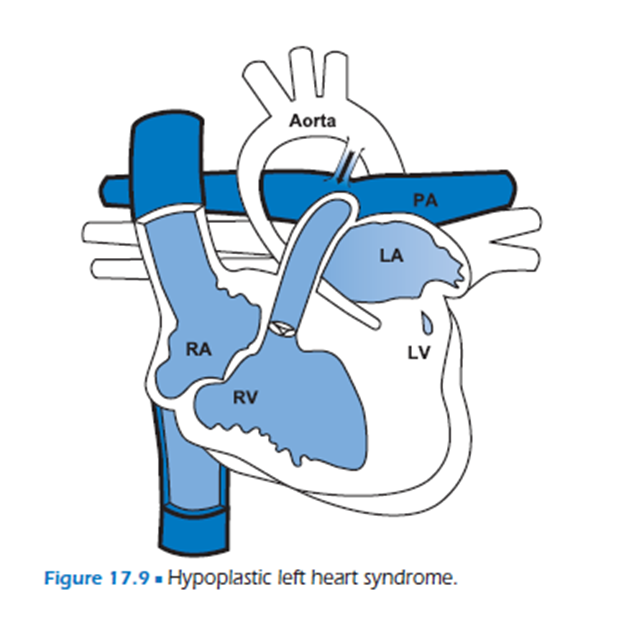
3. Hypoplastic Left Heart Syndrome
Hypoplastic Left Heart Syndrome merupakan kelainan kongenital yang paling serius dengan prognosis yang paling buruk. Cacat ringan didefinisikan sebagai adanya ventrikel kiri yang kecil dengan beberapa penyumbatan. Cacat yang parah didefinisikan sebagai adanya ventrikel kiri yang kecil dan hilangnya katup mitral dan aorta (atresia). Gejalanya biasanya minimal sampai duktus arteriosus menutup dan bayi baru lahir mengalami syok dan kegagalan multiorgan.
Angka kematian pada bayi dengan CHD telah menurun drastis sebagai akibat dari kemajuan medis dan bedah dalam perawatan mereka. Penurunan angka kematian kini telah mengalihkan fokus dari angka kematian ke status perkembangan saraf individu tersebut dan keterlambatan perkembangan yang terkait dengannya. Oleh karena itu, PJK merupakan hasil dari warisan genetik, kondisi ibu, dan faktor lingkungan, yang berinteraksi selama tahap perkembangan penting jantung—selama 8 hingga 10 minggu pertama kehamilan. Ada banyak jenis CHD, masing-masing memiliki risiko dan frekuensi relatifnya sendiri. Untuk memahami berbagai CHD, kita perlu memiliki pemahaman yang jelas tentang perkembangan jantung normal, anatomi, dan fisiologi.
Baca juga : Anak Belum Mampu Berjalan? Begini Solusinya
Referensi :
- Tecklin, Jan S. 2008. Pediatric Physical Therapy fourth edition. Philadelphia : Lippincott Williams & Wilkins



