
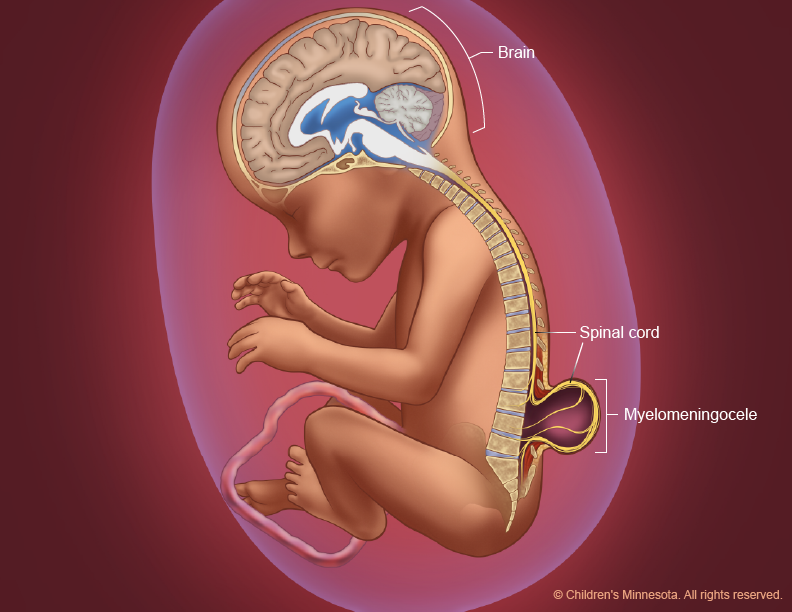
Spina bifida is a birth defect in which the spine does not close. It is usually caused by the failure of the embryo's neural tube to close in the fourth week after conception. The most common type of spina bifida is myelomeningocele (MMC), where the spinal cord opens toward the back and forms a plaque on the back of the fetus.

Individuals with MMC often exhibit motor and sensory neurological deficits below the level of the lesion. This typically results in weakness or paralysis of the lower extremities, which can impede walking and reduce sensation, increasing the risk of injury. Orthopedic abnormalities such as talipes, contractures, hip dislocation, scoliosis, and kyphosis are also common in MMC cases.
Risk Factors
Faktor risiko potensial terjadinya spina bifida adalah :
- Maternal nutrition
- Alcohol use
- Use of caffeine
- Low folate intake
- Poor food quality
- Increased glycemic load
- Low methionine intake
- Low serum choline levels
- Low serum vitamin b12 levels
- Low zinc intake
- Other maternal factors
- Smoke
- Hyperthermia
- Low socioeconomic status
- Maternal infections and diseases
- Diabetes (pregestational insulin dependence)
- Obesity
- Psychosocial stress
- Use of valproic acid
- Environment
- Air pollution
- Disinfectant by-products in beverages
- Indoor air pollution
- Compounds related to nitrate
- Organic solvents
- Pesticide
- Polycyclic aromatic hydrocarbons
Etiology
The primary disorder of MMC is the failure of neural tube closure in the embryonic spinal cord region, which causes the open neural tube to be exposed to the amniotic fluid environment for too long. However, over time, the spinal cord becomes hemorrhagic and neurons die due to amniotic fluid toxicity. Axonal connections eventually break down and lose their function. Neurological defects in MMC are thought to be due to failure of neural tube closure followed by neurodegeneration in utero.
Postnatal Pathogenesis
MMC is a common form of spina bifida and is associated with cerebral malformations and hydrocephalus. The primary brain defect involves a spectrum of anomalies associated with Chiari II malformation of the hindbrain. This is associated with a normal-sized cerebellum developing in a small posterior fossa, resulting in the cerebellum herniating downward through the foramen magnum. On quantitative macrostructural assessment, the hippocampus (but not the amygdala) has decreased volume and an enlarged putamen. Approximately one-third to one-half of children with MMC have hypogenesis (underdevelopment) of the corpus callosum involving the splenium and posterior corpuscles. These abnormalities suggest that the neuronal migration disturbance in MMC persists into the second trimester, since the corpus callosum develops from 8 to 20 weeks before birth.
A secondary consequence of MMC is hydrocephalus caused by cerebrospinal fluid obstruction at the level of the fourth ventricle. Hydrocephalus has a linear effect on cognitive and motor outcomes, reflecting the severity of white matter impairment.
Attention deficits are common in MMC, reflecting problems with the posterior attention system involving midbrain-mediated orientation and arousal, with tectal anomalies directly correlating with the degree of stimulus control difficulties. In contrast, motor functions such as procedural learning and attention functions involving sustained attention and persistence are relatively preserved. This likely reflects less impairment in frontal-striatal and basal ganglia regions. Anomalies in the corpus callosum are associated with reduced interhemispheric communication and more general difficulties in integrating information in language, reading, and social domains.
Neurocognitive impairment can be observed from 6 months to 2 years of age. It reflects general domain deficits in timing, attention, and movement that affect the development of people with MMC throughout life. This results in difficulties in learning to construct and assimilate information (assembly processing) in contrast to relative strengths in associative and procedural learning (associative processing).
Intellectual disability is relatively rare in MMC, and often occurs as a complication of hydrocephalus. The characteristics of the cognitive strengths and weaknesses associated with MMC vary widely and are not well reflected in IQ scores. Strengths reflect preservation of associative processing including procedural learning, word reading, vocabulary and language forms, persistence and social activation. This contrasts with weaknesses in motor adaptation, language comprehension and pragmatics, and hypersociality. Cognitive and motor outcomes are directly related to the level of spinal cord lesion, reflecting the association between more severe brain dysmorphology and higher levels of disability.
Also read: Congenital Heart Defect: Recognize Heart Abnormalities in Babies
Reference :
- Copp, A., Adzick, N., Chitty, L. dkk. Spina bifida. Nat Rev Dis Primer 1 , 15007 (2015). https://doi.org/10.1038/nrdp.2015.7



